




WRITTEN BY PROF ANTHONY NWORAH
Marriage breakdown is now the order of the day. In those days, childlessness was always blamed on the woman. Today, however, it is clear that men are responsible for most of the reproductive failures, owing to sperm problems mainly. Women account for less than forty per cent of the family travails.
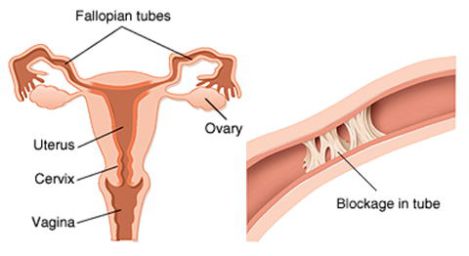
In older women, one can think of other obscurities like fibroids, ovarian tumours, and the sorts, apart from the vacillations of pre-menopause. The commonest cause in young girls is blocked fallopian tubes and backward displacement of the womb. The fallopian tube emanates from the upper sides of the womb, called the uterus, and ends up with finger-like projections on the ovary, which lies on both sides of the uterus. With these fingers, they can pick up the tiny egg, called ovum, laid by the ovary in a process called ovulation. This egg migrates towards the womb.
When the sperms are deposited inside the pelvis, they also start migrating towards the womb en route to the fallopian tubes where they meet with the advancing egg and one of them fuses with it. This is called fertilization, and that is the beginning of pregnancy. The fussed body jointly descends to the womb, settle there and start developing into a full human being over the next nine months when it is been delivered.
When therefore there is a blockage of the tubes, the egg and the sperm cannot meet, and there would be no conception. If one tube is open, the woman may still have a chance of getting pregnant, but only if the ovulating ovary is on the side of the open fallopian tube. Or, by a very rare chance too, the egg migrates from the blocked side to the open side where it can, once more, find access into the tube and meet with the advancing sperm.
Unfortunately, ovulation does not take place between the two ovaries on monthly intervals. One ovary would be ovulating every month for up to three or four years before the other takes over. Therefore, if the ovulation is taking place on the side of the blocked tube, the woman may not conceive until ovulation returns to the ovary of the open tube, unless rare miracles happen. This is why some women get pregnant, without treatment, only once in every three to four years, referred to as “Ime Enyi” in Igbo language. Were the ovaries functioning in monthly turns, there would be no problem as long as one tube is open. If it does not happen in this month, it will happen in the next, but unfortunately the two ovaries do not act on monthly intervals but in 3 to 4 yearly turns.
The causes of tubal blockages are first, infections and by germs, which found their way into the reproductive system from pit toilets, unflushed water toilets, contaminated pads and pants, forgotten tampons, dusts, (usually from women farmers not wearing pants), unclean bathing water, or oral sex, and from contaminated abortions as well as unhygienic delivery rooms and instruments.
Other causes of tubal blockage are compression of the tubes by fibroids and ovarian tumours. This is why it is advisable to do a Tubal flush a couple of months after abdominal operations, particularly fibroids. Also, tubal malformations, ectopic pregnancies and contraceptive tying of tubes add their own sorrows, as to repair the tubes later when pregnancy is once more desired, yields only about ten to twenty percent success, no matter how sophisticated the operation is. The same applies to malformed tubes.
Suspicions are raised when the woman starts complaining of pelvic discomforts, vaginal discharge, or inability to conceive, despite regular itineraries there. There should therefore be series of examinations. A pelvic scan can be added. These investigations are highly recommended to young women before they go into wedlock, so that any abnormal situation could be corrected in time.
Treatments consist of doing a laboratory analysis and culture of the genital organs as well as of the urinary tract. If there are infections, they are aggressively treated before any other thing. If the tubes are blocked from within the lumen of the tube, Tubal flush is carried out, and this consists of mixing a number of drugs as suggested in the lab tests, mixing them with a dissolving agent and then pumping the mixture into the tubes through the womb. If the blockage is from outside the tube, other measures have to be taken, depending on findings. Some may even call for operations, if issues like fibroids, ovarian cysts, massive adhesions, are involved.
Comments are closed for this post.